|
|
| |
 |
|
|
 |
| |
 |
|
USA release new resuscitation guidelines |
|
|
|
 |
| |
|
Both the
European
Resuscitation
Council (ERC)
and the
American
Heart
Association
(AHA) have
this month
released the
2015
International
Resuscitation
Guidelines.
In December
the
Australian
Resuscitation
Council
(ARC) will
release
theirs.
The
Europeans
and
Americans
have ensured
that
simplicity
is the key
issue, which
is evident
when one
reads the
AHA summary
below.
It will be
interesting
to see if
the ARC
guidelines
continue
with its
laboured and
confusing
‘DRSABCD’
algorithm,
instead of
taking a
fresh and
simple
approach to
delivering
basic CPR.
Here are
some of the
AHA
recommendations:
Adult Basic
Life Support
and CPR
Quality: Lay
Rescuer CPR
Summary of
Key Issues
and Major
Changes
Key issues
and major
changes in
the 2015
Guidelines
Update
recommendations
for adult
CPR by lay
rescuers
include the
following:
-
The
crucial
links in
the
out-of-hospital
adult
Chain of
Survival
are
unchanged
from
2010,
with
continued
emphasis
on the
simplified
universal
Adult
Basic
Life
Support
(BLS)
Algorithm.
-
The
Adult
BLS
Algorithm
has been
modified
to
reflect
the fact
that
rescuers
can
activate
an
emergency
response
(ie,
through
use of a
mobile
telephone)
without
leaving
the
victim’s
side.
-
It is
recommended
that
communities
with
people
at risk
for
cardiac
arrest
implement
PAD
programs.
-
Recommendations
have
been
strengthened
to
encourage
immediate
recognition
of
unresponsiveness,
activation
of the
emergency
response
system,
and
initiation
of CPR
if the
lay
rescuer
finds an
unresponsive
victim
is not
breathing
or not
breathing
normally
(eg,
gasping).
-
Emphasis
has been
increased
about
the
rapid
identification
of
potential
cardiac
arrest
by
dispatchers,
with
immediate
provision
of CPR
instructions
to the
caller
(i.e.,
dispatch-guided
CPR).
-
The
recommended
sequence
for a
single
rescuer
has been
confirmed:
the
single
rescuer
is to
initiate
chest
compressions
before
giving
rescue
breaths
(C-A-B
rather
than
A-B-C)
to
reduce
delay to
first
compression.
The
single
rescuer
should
begin
CPR with
30 chest
compressions
followed
by 2
breaths.
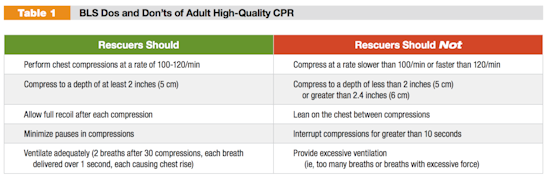
-
There is
continued
emphasis
on the
characteristics
of
high-quality
CPR:
compressing
the
chest at
an
adequate
rate and
depth,
allowing
complete
chest
recoil
after
each
compression,
minimizing
interruptions
in
compressions,
and
avoiding
excessive
ventilation.
-
The
recommended
chest
compression
rate is
100 to
120/min
(updated
from at
least
100/min).
-
The
clarified
recommendation
for
chest
compression
depth
for
adults
is at
least 2
inches
(5 cm)
but not
greater
than 2.4
inches
(6 cm).
-
Bystander-administered
naloxone
may be
considered
for
suspected
life-threatening
opioid-associated
emergencies.
Dispatcher
Identification
of Agonal
Gasps
Cardiac
arrest
victims
sometimes
present with
seizure-like
activity or
agonal gasps
that can
confuse
potential
rescuers.
Dispatchers
should be
specifically
trained to
identify
these
presentations
of cardiac
arrest to
enable
prompt
recognition
and
immediate
dispatcher-guided
CPR. To help
bystanders
recognize
cardiac
arrest,
dispatchers
should
inquire
about a
victim’s
absence of
responsiveness
and quality
of breathing
(normal
versus not
normal). If
the victim
is
unresponsive
with absent
or abnormal
breathing,
the rescuer
and the
dispatcher
should
assume that
the victim
is in
cardiac
arrest.
Dispatchers
should be
educated to
identify
unresponsiveness
with
abnormal and
agonal gasps
across a
range of
clinical
presentations
and
descriptions.
Emphasis on
Chest
Compressions*
Untrained
lay rescuers
should
provide
compression-only
(Hands-Only)
CPR, with or
without
dispatcher
guidance,
for adult
victims of
cardiac
arrest. The
rescuer
should
continue
compression-only
CPR until
the arrival
of an AED or
rescuers
with
additional
training.
All lay
rescuers
should, at a
minimum,
provide
chest
compressions
for victims
of cardiac
arrest. In
addition, if
the trained
lay rescuer
is able to
perform
rescue
breaths, he
or she
should add
rescue
breaths in a
ratio of 30
compressions
to 2
breaths. The
rescuer
should
continue CPR
until an AED
arrives and
is ready for
use, EMS
providers
take over
care of the
victim, or
the victim
starts to
move.
Chest
Compression
Rate*
2015
(Updated):
In adult
victims of
cardiac
arrest, it
is
reasonable
for rescuers
to perform
chest
compressions
at a rate of
100 to
120/min. The
number of
chest
compressions
delivered
per minute
during CPR
is an
important
determinant
of return of
spontaneous
circulation
(ROSC) and
survival
with good
neurologic
function.
The actual
number of
chest
compressions
delivered
per minute,
is
determined
by the rate
of chest
compressions
and the
number and
duration of
interruptions
in
compressions
(eg, to open
the airway,
deliver
rescue
breaths,
allow AED
analysis).
In most
studies,
more
compressions
are
associated
with higher
survival
rates, and
fewer
compressions
are
associated
with lower
survival
rates.
Provision of
adequate
chest
compressions
requires an
emphasis not
only on an
adequate
compression
rate but
also on
minimizing
interruptions
to this
critical
component of
CPR. An
inadequate
compression
rate or
frequent
interruptions
(or both)
will reduce
the total
number of
compressions
delivered
per minute.
New to the
2015
Guidelines
Update are
upper limits
of
recommended
compression
rate and
compression
depth, based
on
preliminary
data
suggesting
that
excessive
compression
rate and
depth
adversely
affect
outcomes.
The addition
of an upper
limit of
compression
rate is
based on 1
large
registry
study
analysis
associating
extremely
rapid
compression
rates
(greater
than
140/min)
with
inadequate
compression
depth. Box 1
uses the
analogy of
automobile
travel to
explain the
effect of
compression
rate and
interruptions
on total
number of
compressions
delivered
during
resuscitation.
|
|
|
Chest
Compression
Depth*
During
manual CPR,
rescuers
should
perform
chest
compressions
to a depth
of at least
5cm for an
average
adult, while
avoiding
excessive
chest
compression
depths
(greater
than 6 cm).
Compressions
create blood
flow
primarily by
increasing
intrathoracic
pressure and
directly
compressing
the heart,
which in
turn results
in critical
blood flow
and oxygen
delivery to
the heart
and brain.
Rescuers
often do not
compress the
chest deeply
enough
despite the
recommendation
to “push
hard.” While
a
compression
depth of at
least 2
inches (5
cm) is
recommended,
the 2015
Guidelines
Update
incorporates
new evidence
about the
potential
for an upper
threshold of
compression
depth
(greater
than 2.4
inches [6
cm]), beyond
which
complications
may occur.
Compression
depth may be
difficult to
judge
without use
of feedback
devices, and
identification
of upper
limits of
compression
depth may be
challenging.
It is
important
for rescuers
to know that
the
recommendation
about the
upper limit
of
compression
depth is
based on one
very small
study that
reported an
association
between
excessive
compression
depth and
injuries
that were
not life
threatening.
Most
monitoring
via CPR
feedback
devices
suggests
that
compressions
are more
often too
shallow than
they are too
deep.
Bystander
Naloxone in
Opioid-Associated
Life
Threatening
Emergencies*
For patients
with known
or suspected
opioid
addiction
who are
unresponsive
with no
normal
breathing
but a pulse,
it is
reasonable
for
appropriately
trained lay
rescuers and
BLS
providers,
in addition
to providing
standard BLS
care, to
administer
intramuscular
(IM) or
intranasal
(IN)
naloxone.
Opioid
overdose
response
education
with or
without
naloxone
distribution
to persons
at risk for
opioid
overdose in
any setting
may be
considered.
This topic
is also
addressed in
the Special
Circumstances
of
Resuscitation
section.
There is
substantial
epidemiologic
data
demonstrating
the large
burden of
disease from
lethal
opioid
overdoses,
as well as
some
documented
success in
targeted
national
strategies
for
bystander-administered
naloxone for
people at
risk. In
2014, the
naloxone
auto
injector was
approved by
the US Food
and Drug
Administration
for use by
lay rescuers
and HCPs.
The
resuscitation
training
network has
requested
information
about the
best way to
incorporate
such a
device into
the adult
BLS
guidelines
and
training.
This
recommendation
incorporates
the newly
approved
treatment.
|
|
|
|
|
|
|
|
Australia urged to take
resuscitation seriously |
|
|
|
|
|
| |
Australia
urged to
take
resuscitation
seriously
This article
was
originally
published on
22 January
2013. Please
note that
Professor
Jacobs,
mentioned in
this
article,
passed away
earlier this
year.
Australian
Doctor
follows one
emergency
doctor's
campaign to
tackle the
country's
'appalling'
record on
resuscitation.
It's been 23
years since
Kerry Packer
famously
‘returned
from the
dead'.
The six
minutes he
spent
pulseless on
a Sydney
polo field
in 1990,
following a
cardiac
arrest,
became a
defining
moment in
the media
mogul's life
after
paramedics
resuscitated
him using a
defibrillator
— a rarity
in
ambulances
at the time. |
|
|
Packer
later told journalist
Ray Martin he had seen
the other side and there
was "nothing" there — no
heaven and no hell. The
experience moved him to
donate thousands of
dollars to fit out every
NSW ambulance with
defibrillators, so other
lives could be saved.
Eight
years after his death in
2005, Packer's legacy
lives on, with
defibrillators still
fondly known by many as
‘Packer-whackers'.
But it's
become clear that his
near-death experience
represented the high
point of Australia's
interest in
defibrillation and
resuscitation. National
dialogue has dwindled
ever since, with
precious little
government funding or
leadership.
One man
who hopes to reverse
that decline is Paul
Middleton, an emergency
physician at Sydney's
Manly Hospital who
chairs the NSW branch of
the Australian
Resuscitation Council.
"People
need to push things for
them to be on the radar.
And cardiac arrest is
something that gets
lost, really," says
Associate Professor
Middleton.
"Notionally, people know
it's something that can
happen to almost
anybody. They all watch
ER and those programs
about the RPA [Royal
Prince Alfred Hospital]
and The Alfred in
Melbourne, and they
think ‘It's never going
to be me'. But the
problem is it’s going to
be you, or somebody like
you, or somebody next to
you.”
Black
Hole
Roughly
30,000 Australians are
thought to experience a
cardiac arrest each
year, 8% of whom
survive.
About
30-35% of cardiac
arrests are due to
ventricular
fibrillation, and
therefore shockable when
first encountered by
medical staff. Survival
rates are better in this
group, at 20-25%, but
still far short of what
can be achieved when CPR
and defibrillation are
given rapidly.
Have a VF
arrest in the Melbourne
Cricket Ground, for
example, and you have a
71% chance of surviving.
Airports and casinos are
also good places to
arrest: Chicago O'Hare
has reported 75%
survival from VF
arrests, and Las Vegas
casinos 53%.
Professor
Middleton says these
successes could be
replicated on a bigger
scale, with the
appropriate funding,
implementation and
leadership.
He
describes Australia's
survival rate as
"appalling",
particularly since more
than half of cardiac
arrests occur in front
of other people. CPR is
only attempted in
one-third of cases.
NSW in
particular has become a
"black hole" for cardiac
arrest, he says; there
is no directory of
automated external
defibrillators, no
statewide CPR training
program and no
centralised collection
of data to inform
practice.
The only
proper estimate to date
of Sydney's survival
rates, published in
2006, found just 14% of
patients survived a week
after cardiac arrest and
11.5% survived a year.
Professor Middleton is
working on a new study
that suggests overall
survival has declined
since then, although the
reasons for this are
unclear.
Having
attended some 500
out-of-hospital cardiac
arrests in his 20-year
career, arriving "almost
always too late", he
believes a concerted,
system-wide drive is
needed to ensure
effective CPR and
defibrillation are given
quicker in the
community.
He
estimates 90% of the
arrests he has attended
were fatal, with the
window for intervention
often missed as family
members or bystanders
watched on, helpless.
"We can
improve all we want in
hospitals, but we'll
still have 10% survival
and 90% death rates
until we realise that
it's not in my hands —
it's in the hands of the
bloke's wife standing
next to him,” Professor
Middleton says.
"I've
been to endless scenes
where there's so much
that could have been
done with minimal
amounts of training.
People often say they
thought about doing CPR
but didn't, because they
thought they would be
causing harm. Okay,
occasionally you can
break a rib, but isn't
it better to have a
broken rib and be alive
than have an intact
chest and be dead?"
CPR is
now easier than ever to
perform, he adds, with
mouth-to-mouth no longer
considered mandatory.
Guidelines still
recommend it where
possible, but have
acknowledged since 2010
that continuous,
compression-only CPR is
a viable alternative to
traditional CPR. Indeed
some studies have
suggested it might even
be superior.
Chain
of survival
It's a
different mood over in
Victoria, which
continues to lead the
way for cardiac arrest
care in Australia.
Statewide, 30% of people
survive to hospital
discharge after an
out-of-hospital
ventricular
tachycardia/ventricular
fibrillation arrest and
11% after any cardiac
arrest.
Associate
Professor Tony Walker, a
paramedic and Ambulance
Victoria's general
manager of regional
services, says these
outcomes are the best in
the country and in the
top 5% worldwide. This
success reflects a
concerted effort to
shape the entire
emergency response
system around the "chain
of survival", ensuring
that every link is as
fast and effective as
possible, he says.
"The
ambulance service across
the country is fantastic
but the difference is
that we've really
focused on cardiac
arrest, and we do a lot
of clinical research to
inform improvement. We
measure it, and we're
all held accountable for
those measures."
Community
recognition of cardiac
arrest has been raised
in Victoria through the
4 Steps for Life
program, which has
taught about one million
people to recognise
cardiac arrest, call
triple-0 and perform
CPR. The program has
just launched iPhone and
iPad apps to guide
bystanders through the
process.
Ambulance
Victoria has meanwhile
reshuffled its dispatch
systems to ensure
suspected cardiac
arrests are assigned the
highest priority. It
also harnesses other
emergency services; in
Melbourne, firefighters
carry defibrillators and
oxygen, are fully
trained in CPR and can
be dispatched to calls
if they are closer than
an ambulance. This
program is being piloted
across the state.
In rural
areas, survival rates
from VT/VF arrest have
risen dramatically since
2008 when the
Metropolitan Ambulance
Service, Rural Ambulance
Victoria and the
Alexandra District
Ambulance Service merged
into a single provider,
enabling them to
harmonise their systems.
Forty-two per cent of
rural patients now
survive to hospital and
17% to discharge, up
from 23% and 7%,
respectively, in 2007.
Crucially, Victoria is
also home to Australia's
largest cardiac arrest
registry, which has now
captured data on 60,000
cases, Professor Walker
says.
Community pride
Internationally,
Australia's survival
rates from cardiac
arrest are "middle of
the road". "We're not
lagging behind but we've
got capacity to improve
substantially," says Ian
Jacobs, professor of
resuscitation and
pre-hospital care at the
University of WA and
chair of the national
Australian Resuscitation
Council.
The
global benchmark is
Seattle, with survival
rates from VF cardiac
arrest as high as 40%.
"They
have a wide community
education program, and
there's a lot of pride
in being the world's
best place to have a
cardiac arrest. They
also have very
sophisticated response
systems ... and a very
aggressive approach to
resuscitation care."
The
whole-of-community
approach is also being
ramped up in WA, where a
St John Ambulance-led
program has provided
automated external
defibrillators,
community education and
first aid courses to
about 150 small towns
across the state, says
Professor Jacobs, who is
also clinical services
director at St John
Ambulance, WA.
The
program has also trained
up about 300 ‘first
responders' — designated
members of the public
who are dispatched to
nearby cardiac arrests.
"The
community is the
ultimate coronary care
unit. If you've got a
trained community that
can do CPR and shock,
that's [as good as] a
first responder
program."
A new
direction to take
Similar
community-focused
projects exist in other
Australian states, to
varying degrees, he
adds.
As well
as raising public
awareness, Australia
will need to address its
lack of automated
external defibrillator
directories if it is to
boost cardiac arrest
survival.
The
devices are thought to
be commonplace,
particularly in shopping
centres and sports
clubs, but they're as
good as useless if they
can't be found and used
within minutes.
Ambulance
Victoria runs a
directory that allows
triple-0 operators to
tell callers if there is
a defibrillator on site
they can use. It has
around 1000
defibrillators
registered but even this
is incomplete, since the
system depends on owners
to be proactive and log
their defibrillators.
Outside
Victoria, Professor
Jacobs says he has "no
clue whatsoever" how
many devices are in
Australia, or where to
find them. He has,
however, been freshly
inspired by a recent
‘crowd sourcing' project
in Philadelphia, which
made a public
competition out of
finding and
photographing automated
external defibrillators.
"I don't
see why we couldn't do
that here," says
Professor Jacobs. "It's
an excellent way of
getting the
information."
Winning hearts and minds
Back in
Sydney, Professor
Middleton is gearing up
for a publicity
offensive to finally get
resuscitation back on
the agenda.
The
Australian Resuscitation
Council NSW, a
voluntary,
not-for-profit group
that has traditionally
focused on training
health professionals, is
now financially and
structurally ready to
step up its public
profile and attempt to
influence policy, he
says.
Several
organisations, including
St John Ambulance and
the Red Cross, run basic
life support and CPR
training courses, but
what's truly needed is a
statewide,
government-sponsored
program, Professor
Middleton says.
He also
wants serious financial
commitment to public
access defibrillation
programs in regional
towns and cities as well
as Sydney. There has
recently been some good
news on this front, with
the Red Cross launching
a new national
initiative called
Project Defib, to
subsidise defibrillators
in sports clubs.
Nationally, there is
also fresh optimism in
the form of a recent
$2.5 million, five-year
NHMRC grant — the first
serious injection of
federal funds into
out-of-hospital cardiac
arrest research for
years. The money has
been used to establish
Aus-ROC, the Australian
Resuscitation Outcomes
Consortium, which has
brought together several
experts to conduct
multicentre clinical
trials, examine existing
systems and build
capacity.
Aus-ROC
also plans to join
existing cardiac arrest
registries in Victoria,
SA and WA into one
super-registry, which
could turn Australia
into a world leader for
resuscitation research.
"It's
getting some momentum.
This is the first real
effort to get
out-of-hospital cardiac
arrest onto the research
agenda and to be able to
inform policy and
practice," says
Professor Jacobs, an
Aus-ROC chief
investigator.
Professor
Middleton says he is
"under no illusions"
that it will be quick or
easy to get Australians
fully engaged with
resuscitation.
"All
we've ever had is that
single, high-profile
event," he says of
Packer's cardiac arrest.
"But it needs to be a
whole public health
campaign. We've got 23
million people in
Australia — a big chunk
of them will die of a
cardiac arrest, and at
government level there's
very little being done."
|
|
|
|
| |
|
|
|
Continuous chest
compressions as
effective as standard
CPR |
|
|
|
|
|
| |
Resuscitation
Outcomes
Consortium
study of
out-of-hospital
cardiac
arrest found
little
difference
in
neurologically
intact
survival
BIRMINGHAM,
Ala. –
Continuous
chest
compression,
touted as
the new way
to perform
cardiopulmonary
resuscitation,
was not an
improvement
over
standard
CPR,
according to
findings
published in
the New
England
Journal of
Medicine
Nov. 9.
Eight U.S.
and Canadian
universities
were
involved the
Resuscitation
Outcomes
Consortium
(ROC) study,
which was
the largest
ever
conducted on
out-of-hospital
cardiac
arrest. |
|
|
The study
looked at more than
23,000 adults with
out-of-hospital cardiac
arrest, for whom EMS
crews responded. Those
patients were randomized
in the eight
participating
communities to either
standard CPR or
continuous chest
compression.
Standard
CPR is 30 chest
compressions with a
pause for two
ventilations, or
breaths. Continuous
chest compression (CCC)
CPR is uninterrupted
chest compressions with
one ventilation every 10
compressions without
pausing compressions
while ventilating the
patient.
"We
did not see any
significant difference
in neurologically intact
survival to hospital
discharge between
patients receiving
standard 30:2 CPR
compared to those
receiving CCC," said
Henry Wang, study
co-author and professor
in the University of
Alabama at Birmingham (UAB)
Department of Emergency
Medicine. "The
neurologically intact
survival rate for
patients receiving 30:2
CPR was 7.7 percent,
against 7 percent for
those receiving CCC."
The
neurologically intact
standard means that,
upon discharge from the
hospital, a patient has
no significant cognitive
deficit and can return
to near-normal function.
"There
have been some
smaller-scale studies
that suggest CCC was as
effective or perhaps
more effective than
30:2; but until now,
that had never been
tested in a full-scale,
randomized clinical
trial," Wang said.
"The current results
indicate that 30:2 and
CCC are equally
effective. Further
evaluation of the role
of ventilation in CPR is
warranted."
Wang says
that, over the past 10
years, CCC has been
suggested as an easier
and safer way for an
individual to perform
CPR.
"In
the absence of
differences in patient
outcomes between the two
CPR strategies, the
study’s conclusion is
that EMS practitioners
and their medical
directors should decide
on an individual basis
if they will perform
30:2 or continuous chest
compressions," said
Shannon Stephens, an
instructor in the UAB
Department of Emergency
Medicine and a study
co-author.
The ROC
CCC trial, which began
in June 2011 and ran
through May 2015, was
carried out in
Birmingham; British
Columbia; Dallas; King
County, Washington;
Milwaukee; Ottawa,
Ontario; Toronto and
Pittsburgh.
Editor’s Note: First
Response Australia (FRA)
plans to launch a local
community based program
to encourage all
citizens to understand
the benefits of
‘Compression only CPR’.
The program will be
called ‘CPR tips without
the lips’. FRA will be
looking to local
government and
businesses to support
the campaign to get the
message out to the
community. The campaign
will include,
distribution of posters
and wallet cue cards
along with public
demonstration.
Unfortunately, since the
arrival of ‘accredited ‘
training requirements,
the standard of CPR
training has declined
dramatically and the
message of simplicity
regarding CPR has been
lost.
Charles Makray
|
|
|
|
|
|
|
|
|
Medic saves shark attack
victim with a boogie
board string |
|
|
|
|
|
| |
Vacationing
medic Marie
Hildreth
used a
boogie board
string as a
tourniquet
for the
12-year-old’s
arm, and a
string from
a beach tent
to stop the
bleeding on
her leg.
OAK ISLAND,
N.C. —
Vacationing
Charlotte
resident and
paramedic
Marie
Hildreth was
throwing a
football
with family
members in
the Oak
Island surf
Sunday when
someone ran
down the
beach
yelling to
get out of
the water
because of a
shark
attack.
"At first I
was like,
'Whatever, a
shark attack
here?' "
Hildreth
said. Even
when a crowd
gathered
around the
victim,
Hildreth's
first
thought was
that the
attack could
just be
lacerations
and cuts
like the
attack on a
girl
reported
Thursday at
Ocean Isle
Beach. |
|
 |
"But
then when I
got there
and saw how
severe the
wounds were,
muscle
memory just
kicked in
and I went
to work like
I normally
do,"
Hildreth
said
Hildreth
created
makeshift
tourniquets
for
12-year-old
shark attack
victim
Kiersten Yow
of Archdale,
who had part
of her left
arm bitten
off and
injuries to
a leg.
After she
identified
herself as a
paramedic,
she said,
she worked
with the
victim's
parents and
other law
enforcement
and fire
officials
who arrived.
Hildreth
grabbed a
boogie board
string and
used it as a
tourniquet
for Yow's
arm. Another
bystander
grabbed a
string from
a beach
tent, which
Hildreth
used to stop
the bleeding
on the
victim's
leg.
In a news
release, New
Hanover
Regional
Medical
Center said
Kiersten
lost her arm
below the
elbow after
the shark
attack and
suffered
tissue
damage to
her leg. She
was
transferred
to another
hospital
Monday for
treatment
after
surgery at
NHRMC.
Hospital and
town
officials
credited
Hildreth and
other first
responders
with helping
to save the
lives of
Kiersten and
Hunter
Treschl, 16,
of Colorado
Springs,
Colo., the
victim of a
second shark
attack
minutes
later and 2
miles away.
Hunter is in
New Hanover
Regional
Medical
Center after
surgery to
repair his
amputated
arm.
Hildreth
can be seen
in news
photos
helping
after the
first
attack, with
a boogie
board just
above
Kiersten's
head. Those
photos,
which have
circulated
across the
world via
The
Associated
Press, were
taken by
vacationer
Steve Bouser,
an editor at
The Pilot
newspaper in
Southern
Pines.
According to
the Shelby
Star, Bouser
and his wife
described a
normal beach
scene that
quickly
turned into
pandemonium.
Brenda
Bouser told
the Shelby
Star the
real heroes
were those
bystanders
who took
quick
action.
"I'm not
sure if it
was her dad
that brought
her on the
beach, but
three young
men and one
woman
swooped in
and took
over,"
Bouser said.
Then,
describing
Hildreth,
Bouser said
a woman who
had a
medical
background
was "barking
orders for a
makeshift
tourniquet."
Steve Bouser
began taking
photos and
documenting
the quick
action of
the
bystanders,
the
emergency
responder's
arrival and
departure
with Yow.
Hildreth,
who has
family on
Oak Island
and loves to
visit, said
the shark
attacks will
not keep her
from coming
back to Oak
Island in
the future.
“But I am
just going
to stay
ankle-deep
in the water
this week,"
she said.
Source:
McClatchy-Tribune
News Service
Editor’s
Note:
Australia
has recently
seen and
increase in
shark
attacks.
Unfortunately,
in many
instances,
lay
responders
attempting
the assist
the victims
are
confronted
with quite a
complex
situation
that basic
first aid
training
does not
equip the
rescue with
the skills
to deal with
such events.
It’s time
that the
likes of
lifesavers
and other
responders,
who may
often be the
first
responders
in such
situations
are equipped
with skills
and
knowledge
that may
save the
victims of
shark
attack.
Responders
need to be
equipped
with
commercial
tourniquets,
specialised
haemostatic
clotting
agents to
immediately
control
severe
external
haemorrhage
, along with
‘Impedance
Threshold
Devices’ to
help
maintain
blood
pressure,
which
dramatically
drops when
such amounts
of blood is
lost.
These skills
and use of
specialised
equipped are
easily
taught to
lay
rescuers,
but because
they are not
mainstream
subjects
taught in
First Aid,
they are
either not
even
considered
for these
circumstances,
or sadly
they are not
even known
about.
Charles Makray
|
|
|
|
|
|
|
|
|
Are there
alternatives to
Emergency Triple Zero
(000)? |
|
|
|
|
|
| |
Australia’s
primary
emergency
call service
number is
Triple Zero
(000), which
can be
dialled from
any fixed or
mobile
phone, pay
phones and
certain
Voice over
Internet
Protocol (VoIP)
services.
There are
also two
secondary
emergency
call service
numbers -
112 and 106.
112 is
available
from all GSM
or GSM
derived
mobile
phones. 106
connects to
the
text-based
relay
service for
people who
have a
hearing or
speech
impairment.
All calls to
the
emergency
numbers,
whether from
fixed,
mobile, pay
phones or
VoIP
services are
free-of-charge.
The
Australian
Communications
and Media
Authority (ACMA)
has produced
a webpage of
frequently
asked
questions on
the
Emergency
Call
Service.
For more
information
on the 106
Text
Emergency
Relay
Service,
Triple Zero
(000) by
internet
relay and
Triple Zero
(000) by
Speak and
Listen, go
to the
National
Relay
Service
website.
|
|
 |
106 - Text
Emergency
Relay
Service
If you have
a hearing or
speech
impairment
and your
life or
property is
in danger,
you can
contact
police, fire
or ambulance
on 106
directly
through a
TTY (also
known as a
teletypewriter
or text
phone). It
is not
possible to
contact
emergency
services
using the
Short
Message
Service (SMS)
on your
mobile
telephone.
The
Australian
106 Text
Emergency
Relay
Service is
provided as
part of the
National
Relay
Service (NRS).
The service
is available
24 hours a
day, 365
days a year
and calls
made using
the 106
service are
given
priority
over other
NRS calls.
Using the
106 Text
Emergency
Relay
Service
Dial 106,
which is a
toll-free
number you
will be
asked if you
want police
(type PPP),
fire (FFF)
or ambulance
(type AAA).
Note Speak
and Listen
(or voice
carry over)
users just
need to say
'police',
'fire' or
'ambulance'
to the relay
officer.
The relay
officer will
dial the
correct
service and
stay on the
line to
relay your
conversation.
As a TTY is
connected to
a fixed
line, the
emergency
service can
locate where
you are
calling from
- You will
be asked to
confirm your
address.
The 106
service can
only be
dialled from
a TTY, it
cannot be
used by:
- An
ordinary
phone
- text
message (SMS)
on a mobile
phone, or
internet
relay.
If you have
further
questions
you can
contact the
National
Relay
Service Help
Desk
(Monday to
Friday 9am
to 5pm AEST)
|
When calling
from a
mobile
telephone
Triple Zero
(000) is
Australia's
primary
telephone
number to
call for
assistance
in life
threatening
or time
critical
emergency
situations.
To find out
more about
calling
Triple Zero
(000) from a
mobile
telephone,
visit the
Australian
Communications
and
Media
Authority
website.
112 - International
standard
emergency
number
Triple Zero
(000) is
Australia's
primary
telephone
number to
call for
assistance
in life
threatening
or time
critical
emergency
situations.
Dialling 112
directs you
to the same
Triple Zero
(000) call
service and
does not
give your
call
priority
over Triple
Zero (000).
|
|
 |
112 is an
international
standard
emergency
number which
can only be
dialled on a
digital
mobile
phone. It is
accepted as
a secondary
international
emergency
number in
some parts
of the
world,
including
Australia,
and can be
dialled in
areas of GSM
network
coverage
with the
call
automatically
translated
to that
country’s
emergency
number. It
does not
require a
simcard or
pin number
to make the
call,
however
phone
coverage
must be
available
(any
carrier) for
the call to
proceed.
There is no
advantage to
dialling 112
over Triple
Zero (000).
Calls to 112
do not go to
the head of
the queue
for
emergency
services,
and it is
not true
that it is
the only
number that
will work on
a mobile
phone.
Dialling 112
from a fixed
line
telephone in
Australia
(including
payphones)
will not
connect you
to the
emergency
call service
as it is
only
available
from digital
mobile
phones.
|
Voice over
Internet
Protocol
Voice over
Internet
Protocol (VoIP)
is a
technology
that allows
telephone
calls to be
made over
broadband
Internet
connections.
Some VoIP
providers
may not
provide
access to
emergency
calls, so
check with
your VoIP
provider if
you require
the
emergency
call
service.
For
information
about using
Voice over
Internet
Protocol (VoIP)
visit the
Communications
Alliance
website. |
|
 |
For more
information
on the key
issues to
consider
before
changing to
VoIP is
available on
the
Australian
Communications
and Media
Authority
website.
State and
territory
emergency
service
organisations
Within
Australia,
the
protection
of life and
property is
the
responsibility
of state and
territory
governments.
A number of
Emergency
Services
Organisations
(ESO)
provide
their own
information
on what to
do in an
emergency.
For more
information,
visit the
state and
territory
emergency
services
organisations
page.
911
911 is the
emergency
telephone
number used
in other
countries
such as the
United
States and
Canada. This
number
should not
be used in
an emergency
in
Australia.
If dialled
within
Australia,
this number
will not
re-route
emergency
calls to
Triple Zero
(000).
|
|
|
|
|
|
 |
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
 |
|
|
First
Response Australia Pty Ltd
Specialists in Emergency Care Training & Equipment
PO Box 81N, North Cairns QLD 4870
201 - 205 Bunda Street, Cairns QLD
4870
P
+61 7 4032 2444 | E
admin@firstresponseaustralia.com.au
|
www.firstresponseaustralia.com.au
|
|
|
| |
|
Should you no
longer wish to receive these emails, please unsubscribe
here. Can't see the images? Outlook users - please click to
download pictures and select, "Add to Safe Senders List." For other email
readers, safe senders instructions
here. If you feel this
message was delivered without your consent, please notify us at
admin@firstresponseaustralia.com.au |
| |
|
|
|